
Any views or opinions presented in this article are solely those of the author and do not necessarily represent those of the company. AHP accepts no liability for the content of this article, or for the consequences of any actions taken on the basis of the information provided unless that information is subsequently confirmed in writing.
Introduction
The high cost of health care in the United States is well known, whether expressed at the cost per service, the cost per person or as a percentage of the Gross Domestic Product. The facts are obvious, we in the United States spend a lot on health care. Solutions to this situation have been suggested for many years, but the expensive reality continues. Is it possible that unique characteristics of the American health care environment create special challenges? This article discusses several of the unique aspects of the American health system.
Geographic Diversity
The United States is a diverse country with population centers scattered throughout the country. The mean center of population for the United States currently lies in Missouri.
Exhibit 1: Mean Center of Population
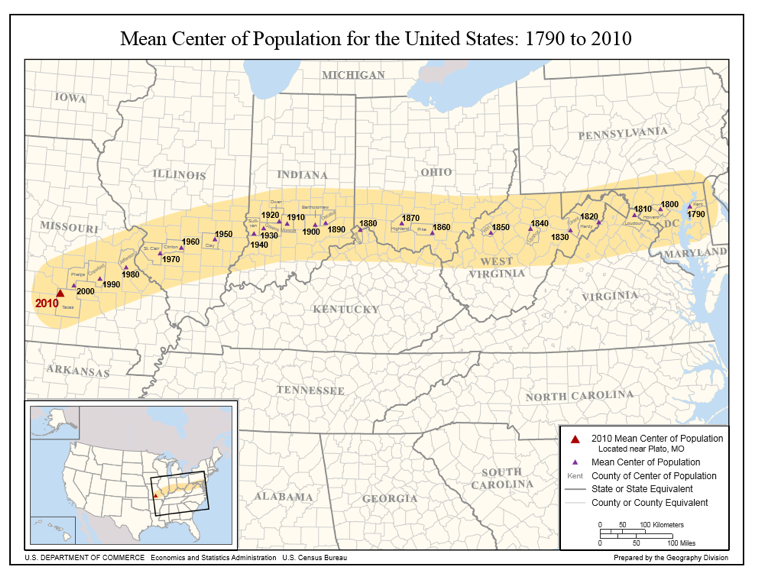
As the inset map shows, this is east and south of the geographic center of the United States. The major population centers in the eastern half of the country pull it east. The major population centers in the south pull it south. More than 10% of the population is in one major southwestern state, California. Major metropolitan areas can be found throughout the country: San Francisco and Los Angeles in the southwest, Dallas and Houston in the south Midwest, Chicago in the upper Midwest, Boston and New York in the northeastern part of the country, Atlanta and Miami in the southeast. Why is this important?
More than 90% of the Canadian population lives within 100 miles of the US border. The often-touted Canadian system serves a population that is concentrated in a thin band of land just north of the US border. The US geographic realities are a consideration that can’t be ignored. In a concentrated environment it is possible to have a more efficient allocation of resources. In the Canadian provinces with significant rural populations (e.g., Alberta and Saskatchewan) the provinces utilize regional health authorities to take responsibility for a specific geographic region.
American Definition of Quality
Quality is difficult to universally define. Many times people say “I know it when I see it” or more importantly “I know it when I don’t see it”. Over the past 15 – 20 years quality has been objectively defined, to the point that it is consistently measured across health systems. Quality metrics are the norm. One of the best definitions of quality is “providing the right service, at the right time, to the right patient as efficiently as possible”. The American definition of quality usually includes a high degree of access and a significant sense of urgency.
Other countries do not associate waiting as a deterioration in quality. In fact queuing or waiting lines are accepted conditions in a health care system. The American ideal is getting their health care now, not tomorrow, not next week, or next year. Most Americans associate waiting as a reduction in quality. Health systems that require pre-authorization or approval of referrals are frequently viewed as substandard since those systems create barriers or hurdles that patients have to work through. In countries with socialized health care systems, patients regularly have to wait for care. Much of this wait is associated with fiscal limits within the system restricting the available resources. In America the excess capacity in the system almost always provides an adequate supply of healthcare resources so the required waiting time is very limited.
The waiting line is caused by either quotas or specific budgets for specific procedures. As the patient moves up the list, they then can be scheduled for the required procedure. The presence of a waiting list or queue is a rigid form of rationing based upon a budget constraint. In the US waiting also occurs but it occurs because the physician was booked or the schedule was full. This queue is not a budget driven constraint.
The US health care system is recognized as one of the highest quality systems in the world (e.g., high cancer screening rates). Although the quality of care is generally quite high, some of the measured outcomes suggest that the US health system is not advancing as much as would be hoped for. One example of this are the efforts to eliminate breast cancer. Screening for breast cancer is higher than it has ever been, but so is the rate of breast cancer. Perhaps improved detection has identified more cases.
Freedom of Choice
Americans value freedom of choice, they like to make decisions for themselves. Americans value going where they want to get care, choosing who they want to provide that care, oftentimes deciding what care they want, and getting it when they want to get it. This has resulted in broader networks offering more choices than needed. This has resulted in higher than necessary utilization of specific services, including new technology. The need for freedom of choice has limited the effectiveness of care management programs. Freedom of choice combined with limited cost sharing results in expensive health care. One unfortunate consequence of the need for freedom of choice is the negative opinion that develops regarding any administrative process that limits freedom of choice. Programs that focus on limiting medically unnecessary care are accused of disrupting the physician/patient relationship. Unrestrained freedom of choice increases the cost of care.
Healthcare Resource Planning
In most states there is very limited overall resource planning efforts. At various times some states have implemented certificate of need programs for specific types of providers. For the most part there are no formal limits to the number of providers or types of providers. In most urban markets there is an oversupply of providers. Rural markets are often plagued with a shortage of providers. Some markets are so desperate for providers significant compensation (i.e., above and beyond what would be considered normal) is offered providers to lure them to that specific market.
Why is this important? Healthcare tends to be a market that fails to respond to traditional supply and demand economics. In the general economy, the greater the supply, the lesser the demand and the lower the prices. In healthcare, the higher the supply, the greater the induced demand and the continuation of higher prices. Informal studies suggest that utilization levels positively correlate with supply (e.g., square root of the physician per capita ratio). One of the reasons for escalating costs is the continued over-supply of health care providers.
Countries with socialized health care systems are much more involved with resource planning than the United States.
One of the best examples of effective resource planning is the approach implemented by Kaiser Foundation Health Plan in its various markets. Kaiser carefully plans the supply of professional services based upon a long-established staffing model. As the associated membership grows, they transition from a combination of “nearby owned facilities” and “rented facilities” to “owned facilities”. They carefully manage the strategic transition to a “wholly owned delivery system” and manage the resources based upon ongoing membership growth. Through this process they avoid excess capacity and as a result maintain a cost effective delivery system.
Countries with socialized health care systems are much more involved with resource planning than the United States. The competitive nature of health care in the United States is much more focused on capturing market share than defining appropriate resources for a region. Less effective resource planning drives up the cost of care since there is a limited demand for services.
Wide Variations in Delivery System Efficiency
The efficiency of regional health care systems varies significant from one geographic market to another. Delivery system care patterns have emerged based upon local needs, regional care practices, and the extent of provider involvement in the financing of care. Markets like Portland, OR have developed extremely efficient inpatient care patterns with a larger portion of their health care dollar going to professional providers. Other markets have emerged at the same time with much less efficient care patterns. Inpatient utilization patterns vary by more than 35% – 45%. Analyses show no clinical rationale to support the observed variation. The United States is one of the few countries exhibiting this level of variation. Experts generally concur that much of this variation is caused by personal physician preference.
Tax Sheltered Benefits
The current tax sheltered employee benefit approach emerged during the post-WWII era where employers were seeking creative ways to attract, hire and keep employees. The tax law enabled employers to write-off the cost of benefits and provide their employees a valuable tax-sheltered employee benefit. The tax law provides this favorable status only to employer sponsored programs. Individual health insurance benefit programs do not enjoy this same tax advantage. Tax reform efforts have considered eliminating this difference. Self-funded employer sponsored benefit programs, including those involving labor union negotiations (i.e., Taft-Hartley plans) are also tax advantaged.
This is an important issue when discussing transitions to alternative systems. What role will employers play? What about labor union negotiated programs? How will we unravel the tax advantaged funding of health care costs by the employer?
Diverse Insurance and Claims Administration
The employee health benefit marketplace has grown significantly with a large variety of organizations targeting the effective administration of such programs. Merger/acquisition activity has transformed the marketplace into a handful of “major players” and a large number of regional players. Third Party Administrators (TPAs) are active in the market supporting the self-funded and self-administered benefit programs. The Federal government provides government sponsored coverage for the elderly and disabled (Medicare) and lower socio-economic level beneficiaries (Medicaid). Many of these programs out-source the administration and risk taking to the private sector. Health care administration in the United States includes a significant private sector involvement. There is little uniformity between different health plans. There are limited standards that streamline the process.
Public/Private Sector Cost Shift
The US health care system incorporates a significant cost shift between the government sponsored programs and the private sector programs. The private sector pays a much higher amount for identical services than the public sector. Within the private sector, each carrier/health plan is required to negotiate payment rates which can vary substantially from one carrier to the next. The variability in reimbursement increases administrative costs for both the providers and the health plans or administrators.
Hesitancy to Declare Health Care as a Human Rights Issue
In the United States there has been a hesitancy to declare health care as a human rights issue. In Canada, the Canada Health Care Act defines five principles:
- Public Administration: All administration of provincial health insurance must be carried out by a public authority on a non-profit basis.
- Comprehensiveness: All necessary health services, including hospitals, physicians and surgical dentists, must be insured.
- Universality: All insured residents are entitled to the same level of health care.
- Portability: A resident that moves to a different province or territory is still entitled to coverage from their home province during a minimum waiting period. This also applies to residents which leave the country.
- Accessibility: All insured persons have reasonable access to health care facilities. In addition, all physicians, hospitals, etc., must be provided reasonable compensation for the services they provide.
A quick internet review will show considerable discussion that defends both opinions, it is a right or it isn’t a right. Dominant emerging thought focuses on what is called Triple Aim1. A strong focus on quality and customer satisfaction, improving the population’s health status and reducing costs the cost are admirable goals, but all require the definition or identification of a population. Who is the population? Is it everyone? Is it just the segment I am concerned about?
Recent health care reform efforts have focused on minimizing uninsured which was a step towards universality. Ironically the American’s demand for freedom of choice also includes freedom from being told that they must buy insurance and what kind of care they should pay for.
Summary
These nine issues provide an initial list of unique characteristics of the US health care system. There are more that could be described. Solutions to resolving the high cost of care must consider these.
1improving the individual experience of care; improving the health of populations; and reducing the per capita costs of care for populations.
About the Author

David Axene, FSA, FCA, CERA, MAAA, is the President and Founding Partner of Axene Health Partners, LLC and is based in AHP’s Murrieta, CA office.